
Identification of Functional Cortical Plasticity in Children with Cerebral Palsy Associated to Robotic-Assisted Gait Training: An fNIRS Study
 , ,
, ,  , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Particpants
- Gross Motor Function Measure-88 (GMFM-88): it consists of 88 items in five dimensions: lying and rolling (GMFM-A); sitting (GMFM-B); crawling and kneeling (GMFM-C); standing (GMFM-D); and walking, running and jumping (GMFM-E) [19].
- Modified Ashworth Scale (MAS): it was developed by Bryan Ashworth as a method of grading spasticity. The original Ashworth scale was a 5 points numerical scale that graded spasticity from 0 to 4, with 0 being no resistance and 4 being a limb rigid in flexion or extension. However, Bohannon and Smith modified the Ashworth scale by adding 1+ to the scale to increase sensitivity. Hence, MAS varies from 0 (no increase in muscle tone) to 4 (affected part(s) rigid in flexion or extension) [20].
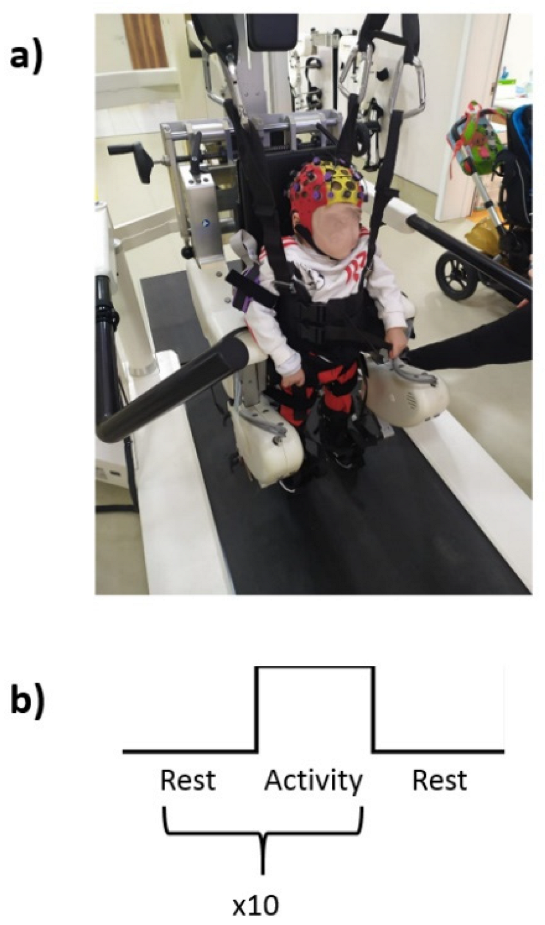
2.2. Experimental Procedure
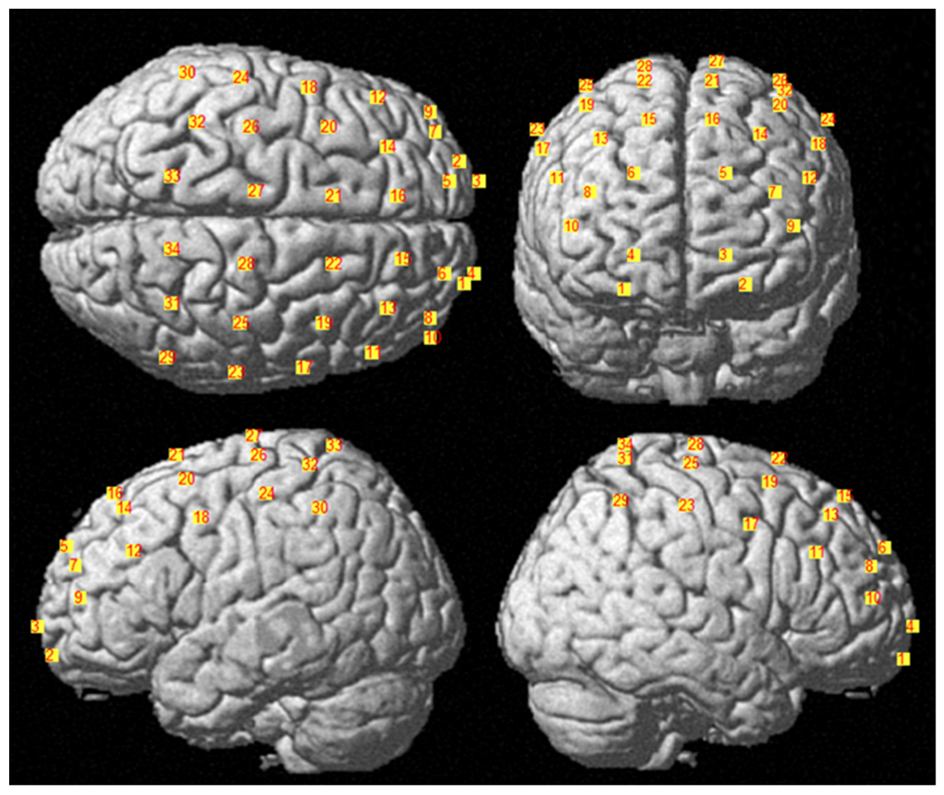
2.3. fNIRS Measurements and Data Analysis
3. Results
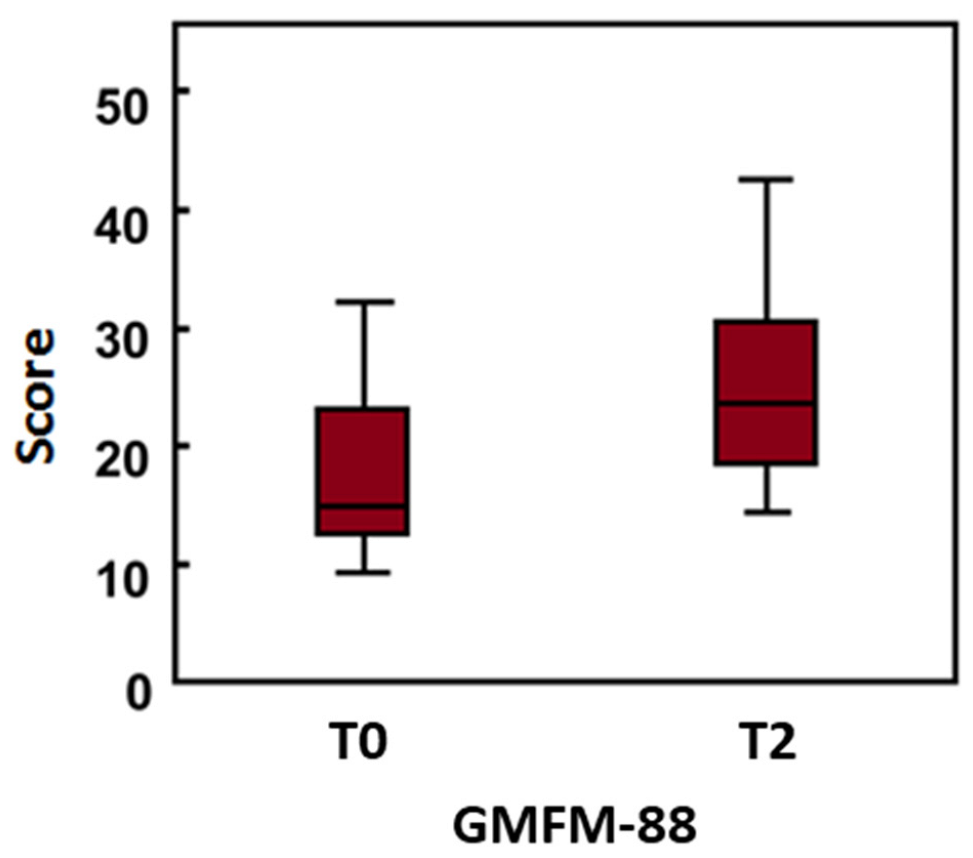
3.1. Clinical Scales Results
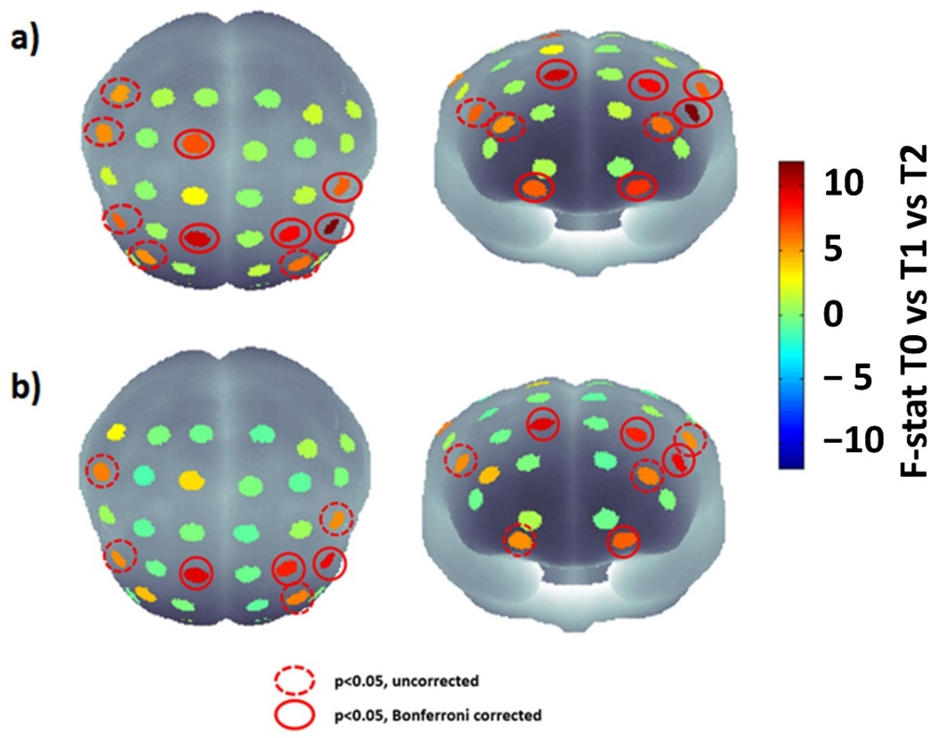
3.2. fNIRS Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Cherni, Y.; Ballaz, L.; Lemaire, J.; Dal Maso, F.; Begon, M. Effect of Low Dose Robotic-Gait Training on Walking Capacity in Children and Adolescents with Cerebral Palsy. Neurophysiol. Clin. 2020, 50, 507–519. [Google Scholar] [CrossRef] [PubMed]
- Sadowska, M.; Sarecka-Hujar, B.; Kopyta, I. Cerebral Palsy: Current Opinions on Definition, Epidemiology, Risk Factors, Classification and Treatment Options. Neuropsychiatr. Dis. Treat. 2020, 16, 1505–1518. [Google Scholar] [CrossRef] [PubMed]
- Palisano, R.J.; Cameron, D.; Rosenbaum, P.L.; Walter, S.D.; Russell, D. Stability of the Gross Motor Function Classification System. Dev. Med. Child Neurol. 2006, 48, 424–428. [Google Scholar] [CrossRef] [PubMed]
- Blackman, J.A.; Svensson, C.I.; Marchand, S. Pathophysiology of Chronic Pain in Cerebral Palsy: Implications for Pharmacological Treatment and Research. Dev. Med. Child Neurol. 2018, 60, 861–865. [Google Scholar] [CrossRef] [PubMed]
- Novak, I.; Morgan, C.; Adde, L.; Blackman, J.; Boyd, R.N.; Brunstrom-Hernandez, J.; Cioni, G.; Damiano, D.; Darrah, J.; Eliasson, A.-C.; et al. Early, Accurate Diagnosis and Early Intervention in Cerebral Palsy: Advances in Diagnosis and Treatment. JAMA Pediatr. 2017, 171, 897–907. [Google Scholar] [CrossRef]
- Schwartz, I.; Meiner, Z. Robotic-Assisted Gait Training in Neurological Patients: Who May Benefit? Ann. Biomed. Eng. 2015, 43, 1260–1269. [Google Scholar] [CrossRef]
- Rossignol, S.; Dubuc, R.; Gossard, J.-P. Dynamic Sensorimotor Interactions in Locomotion. Physiol. Rev. 2006, 86, 89–154. [Google Scholar] [CrossRef]
- Billinger, S.A.; Arena, R.; Bernhardt, J.; Eng, J.J.; Franklin, B.A.; Johnson, C.M.; MacKay-Lyons, M.; Macko, R.F.; Mead, G.E.; Roth, E.J.; et al. Physical Activity and Exercise Recommendations for Stroke Survivors. Stroke 2014, 45, 2532–2553. [Google Scholar] [CrossRef] [Green Version]
- Schmartz, A.C.; Meyer-Heim, A.D.; Müller, R.; Bolliger, M. Measurement of Muscle Stiffness Using Robotic Assisted Gait Orthosis in Children with Cerebral Palsy: A Proof of Concept. Disabil. Rehabil. Assist. Technol. 2011, 6, 29–37. [Google Scholar] [CrossRef]
- Grafman, J. Conceptualizing Functional Neuroplasticity. J. Commun. Disord. 2000, 33, 345–356. [Google Scholar] [CrossRef]
- Granild-Jensen, J.B.; Rackauskaite, G.; Flachs, E.M.; Uldall, P. Predictors for Early Diagnosis of Cerebral Palsy from National Registry Data. Dev. Med. Child Neurol. 2015, 57, 931–935. [Google Scholar] [CrossRef]
- Gramigna, V.; Pellegrino, G.; Cerasa, A.; Cutini, S.; Vasta, R.; Olivadese, G.; Martino, I.; Quattrone, A. Near-Infrared Spectroscopy in Gait Disorders: Is It Time to Begin? Neurorehabil. Neural Repair 2017, 31, 402–412. [Google Scholar] [CrossRef] [Green Version]
- Forcione, M.; Chiarelli, A.M.; Davies, D.J.; Perpetuini, D.; Sawosz, P.; Merla, A.; Belli, A. Cerebral Perfusion and Blood–Brain Barrier Assessment in Brain Trauma Using Contrast-Enhanced near-Infrared Spectroscopy with Indocyanine Green: A Review. J. Cereb. Blood Flow Metab. 2020, 40, 1586–1598. [Google Scholar] [CrossRef]
- Pinti, P.; Tachtsidis, I.; Hamilton, A.; Hirsch, J.; Aichelburg, C.; Gilbert, S.; Burgess, P.W. The Present and Future Use of Functional Near-infrared Spectroscopy (FNIRS) for Cognitive Neuroscience. Ann. N. Y. Acad. Sci. 2020, 1464, 5. [Google Scholar] [CrossRef]
- Kurz, M.J.; Wilson, T.W.; Arpin, D.J. An FNIRS Exploratory Investigation of the Cortical Activity during Gait in Children with Spastic Diplegic Cerebral Palsy. Brain Dev. 2014, 36, 870–877. [Google Scholar] [CrossRef] [Green Version]
- Basura, G.J.; Hu, X.-S.; Juan, J.S.; Tessier, A.-M.; Kovelman, I. Human Central Auditory Plasticity: A Review of Functional near-Infrared Spectroscopy (FNIRS) to Measure Cochlear Implant Performance and Tinnitus Perception. Laryngoscope Investig. Otolaryngol. 2018, 3, 463–472. [Google Scholar] [CrossRef] [Green Version]
- Belda-Lois, J.-M.; Mena-del Horno, S.; Bermejo-Bosch, I.; Moreno, J.C.; Pons, J.L.; Farina, D.; Iosa, M.; Molinari, M.; Tamburella, F.; Ramos, A.; et al. Rehabilitation of Gait after Stroke: A Review towards a Top-down Approach. J. Neuroeng. Rehabil. 2011, 8, 66. [Google Scholar] [CrossRef] [Green Version]
- Morris, C.; Bartlett, D. Gross Motor Function Classification System: Impact and Utility. Dev. Med. Child Neurol. 2004, 46, 60–65. [Google Scholar] [CrossRef]
- Salavati, M.; Krijnen, W.P.; Rameckers, E.A.A.; Looijestijn, P.L.; Maathuis, C.G.B.; van der Schans, C.P.; Steenbergen, B. Reliability of the Modified Gross Motor Function Measure-88 (GMFM-88) for Children with Both Spastic Cerebral Palsy and Cerebral Visual Impairment: A Preliminary Study. Res. Dev. Disabil. 2015, 45–46, 32–48. [Google Scholar] [CrossRef]
- Meseguer-Henarejos, A.-B.; Sánchez-Meca, J.; López-Pina, J.-A.; Carles-Hernández, R. Inter- and Intra-Rater Reliability of the Modified Ashworth Scale: A Systematic Review and Meta-Analysis. Eur. J. Phys. Rehabil. Med. 2018, 54, 576–590. [Google Scholar] [CrossRef]
- Brigadoi, S.; Cooper, R.J. How Short Is Short? Optimum Source–Detector Distance for Short-Separation Channels in Functional near-Infrared Spectroscopy. Neurophotonics 2015, 2, 025005. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ye, J.C.; Tak, S.; Jang, K.E.; Jung, J.; Jang, J. NIRS-SPM: Statistical Parametric Mapping for near-Infrared Spectroscopy. Neuroimage 2009, 44, 428–447. [Google Scholar] [CrossRef] [PubMed]
- Scholkmann, F.; Wolf, M. General Equation for the Differential Pathlength Factor of the Frontal Human Head Depending on Wavelength and Age. J. Biomed. Opt. 2013, 18, 105004. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chiarelli, A.M.; Perpetuini, D.; Filippini, C.; Cardone, D.; Merla, A. Differential Pathlength Factor in Continuous Wave Functional Near-Infrared Spectroscopy: Reducing Hemoglobin’s Cross Talk in High-Density Recordings. Neurophotonics 2019, 6, 035005. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pinti, P.; Scholkmann, F.; Hamilton, A.; Burgess, P.; Tachtsidis, I. Current Status and Issues Regarding Pre-Processing of FNIRS Neuroimaging Data: An Investigation of Diverse Signal Filtering Methods within a General Linear Model Framework. Front. Hum. Neurosci. 2019, 12, 505. [Google Scholar] [CrossRef] [Green Version]
- Perpetuini, D.; Cardone, D.; Filippini, C.; Chiarelli, A.M.; Merla, A. A Motion Artifact Correction Procedure for FNIRS Signals Based on Wavelet Transform and Infrared Thermography Video Tracking. Sensors 2021, 21, 5117. [Google Scholar] [CrossRef]
- Sato, T.; Nambu, I.; Takeda, K.; Aihara, T.; Yamashita, O.; Isogaya, Y.; Inoue, Y.; Otaka, Y.; Wada, Y.; Kawato, M. Reduction of Global Interference of Scalp-Hemodynamics in Functional near-Infrared Spectroscopy Using Short Distance Probes. NeuroImage 2016, 141, 120–132. [Google Scholar] [CrossRef] [Green Version]
- Perpetuini, D.; Cardone, D.; Filippini, C.; Chiarelli, A.M.; Merla, A. Modelling Impulse Response Function of Functional Infrared Imaging for General Linear Model Analysis of Autonomic Activity. Sensors 2019, 19, 849. [Google Scholar] [CrossRef] [Green Version]
- Kohavi, R.; John, G.H. Wrappers for Feature Subset Selection. Artif. Intell. 1997, 97, 273–324. [Google Scholar] [CrossRef] [Green Version]
- Strotzer, M. One Century of Brain Mapping Using Brodmann Areas. Clin. Neuroradiol. 2009, 19, 179–186. [Google Scholar] [CrossRef]
- Wallard, L.; Dietrich, G.; Kerlirzin, Y.; Bredin, J. Robotic-Assisted Gait Training Improves Walking Abilities in Diplegic Children with Cerebral Palsy. Eur. J. Paediatr. Neurol. 2017, 21, 557–564. [Google Scholar] [CrossRef]
- van Kammen, K.; Reinders-Messelink, H.A.; Elsinghorst, A.L.; Wesselink, C.F.; Meeuwisse-de Vries, B.; van der Woude, L.H.; Boonstra, A.M.; den Otter, R. Amplitude and Stride-to-Stride Variability of Muscle Activity during Lokomat Guided Walking and Treadmill Walking in Children with Cerebral Palsy. Eur. J. Paediatr. Neurol. 2020, 29, 108–117. [Google Scholar] [CrossRef]
- Sukal-Moulton, T.; de Campos, A.C.; Alter, K.E.; Huppert, T.J.; Damiano, D.L. Relationship between Sensorimotor Cortical Activation as Assessed by Functional near Infrared Spectroscopy and Lower Extremity Motor Coordination in Bilateral Cerebral Palsy. NeuroImage Clin. 2018, 20, 275–285. [Google Scholar] [CrossRef]
- Chaudhary, U.; Hall, M.; Gonzalez, J.; Elbaum, L.; Bloyer, M.; Godavarty, A. Motor Response Investigation in Individuals with Cerebral Palsy Using near Infrared Spectroscopy: Pilot Study. Appl. Opt. AO 2014, 53, 503–510. [Google Scholar] [CrossRef]
- Kane, M.J.; Engle, R.W. The Role of Prefrontal Cortex in Working-Memory Capacity, Executive Attention, and General Fluid Intelligence: An Individual-Differences Perspective. Psychon. Bull. Rev. 2002, 9, 637–671. [Google Scholar] [CrossRef] [Green Version]
- Lefmann, S.; Russo, R.; Hillier, S. The Effectiveness of Robotic-Assisted Gait Training for Paediatric Gait Disorders: Systematic Review. J. Neuroeng. Rehabil. 2017, 14, 1. [Google Scholar] [CrossRef] [Green Version]
- Carvalho, I.; Pinto, S.M.; das Virgens Chagas, D.; Praxedes dos Santos, J.L.; de Sousa Oliveira, T.; Batista, L.A. Robotic Gait Training for Individuals with Cerebral Palsy: A Systematic Review and Meta-Analysis. Arch. Phys. Med. Rehabil. 2017, 98, 2332–2344. [Google Scholar] [CrossRef]
- Sarhan, R.S.; Chevidikunnan, M.F.; Gaowgzeh, R.A.M. Locomotor Treadmill Training Program Using Driven Gait Orthosis versus Manual Treadmill Therapy on Motor Output in Spastic Diplegic Cerebral Palsy Children. J. Health Allied Sci. NU 2014, 4, 010–017. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Participants | 8 |
| Age (years) | 9.88 ± 4.73 |
| Affected side (n) | |
| Unilateral | 1 |
| Bilateral | 7 |
| Cerebral palsy subtype (n) | |
| Spastic | 8 |
| Dyskinetic | 0 |
| Ataxic | 0 |
| Gross Motor Function Classification System (GMFCS) level (n) | |
| I | 1 |
| II | 0 |
| III | 1 |
| IV | 5 |
| V | 1 |
| (T0) Median (IQR) | (T2) Median (IQR) | p Values | |
|---|---|---|---|
| GMFM 88 | 16 (14–23.6) | 24.3 (19.4–30.9) | Z = −2.524; p = 0.008 |
| MAS H | 1 (0.5–2) | 1 (0.75–1) | n.s. |
| MAS K | 2 (0.5–2) | 1 (0–2) | n.s. |
| MAS A | 2 (1–2) | 1 (0.75–1) | n.s. |
| Subj | Gross Motor Function Classification System (GMFCS) Level | Delta between T0 and T2 (%) |
|---|---|---|
| 1 | III | 30.8 |
| 2 | IV | 27.0 |
| 3 | I | 4.1 |
| 4 | IV | 48.3 |
| 5 | IV | 21.0 |
| 6 | IV | 51.9 |
| 7 | V | 44.5 |
| 8 | IV | 31.4 |
| Channels | Brodmann Areas | Comparison | t-Stat | Adjusted p-Value | |
|---|---|---|---|---|---|
| Ch1 | 1-Orbitofrontal area | T0 vs. T2 | −3.747 | 0.020 | |
| Ch2 | 1-Orbitofrontal area | T0 vs. T1 | −3.799 | 0.018 | |
| Ch12 | 46-Dorsolateral prefrontal cortex | T0 vs. T1 | −3.788 | 0.019 | |
| Oxyhemoglobin (HbO) | Ch12 | 46-Dorsolateral prefrontal cortex | T0 vs. T2 | −4.181 | 0.014 |
| Ch14 | 9-Dorsolateral prefrontal cortex | T0 vs. T2 | 5.937 | 0.004 | |
| Ch15 | 9-Dorsolateral prefrontal cortex | T0 vs. T2 | 4.756 | 0.009 | |
| Ch18 | 6-Pre - Motor and Supplementary Motor Cortex | T0 vs. T2 | −4.075 | 0.015 | |
| Ch28 | 4-Primary Motor Cortex | T0 vs. T2 | −4.037 | 0.016 | |
| Ch2 | 1-Orbitofrontal area | T0 vs. T1 | −3.083 | 0.036 | |
| Deoxyhemoglobin | Ch12 | 46-Dorsolateral prefrontal cortex | T0 vs. T1 | −3.471 | 0.026 |
| (HHb) | Ch12 | 46-Dorsolateral prefrontal cortex | T0 vs. T2 | −4.093 | 0.014 |
| Ch14 | 9-Dorsolateral prefrontal cortex | T0 vs. T2 | 5.099 | 0.007 | |
| Ch15 | 9-Dorsolateral prefrontal cortex | T0 vs. T2 | 4.056 | 0.015 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Perpetuini, D.; Russo, E.F.; Cardone, D.; Palmieri, R.; Filippini, C.; Tritto, M.; Pellicano, F.; De Santis, G.P.; Calabrò, R.S.; Merla, A.; et al. Identification of Functional Cortical Plasticity in Children with Cerebral Palsy Associated to Robotic-Assisted Gait Training: An fNIRS Study. J. Clin. Med. 2022, 11, 6790. https://doi.org/10.3390/jcm11226790
Perpetuini D, Russo EF, Cardone D, Palmieri R, Filippini C, Tritto M, Pellicano F, De Santis GP, Calabrò RS, Merla A, et al. Identification of Functional Cortical Plasticity in Children with Cerebral Palsy Associated to Robotic-Assisted Gait Training: An fNIRS Study. Journal of Clinical Medicine. 2022; 11(22):6790. https://doi.org/10.3390/jcm11226790
Chicago/Turabian StylePerpetuini, David, Emanuele Francesco Russo, Daniela Cardone, Roberta Palmieri, Chiara Filippini, Michele Tritto, Federica Pellicano, Grazia Pia De Santis, Rocco Salvatore Calabrò, Arcangelo Merla, and et al. 2022. "Identification of Functional Cortical Plasticity in Children with Cerebral Palsy Associated to Robotic-Assisted Gait Training: An fNIRS Study" Journal of Clinical Medicine 11, no. 22: 6790. https://doi.org/10.3390/jcm11226790